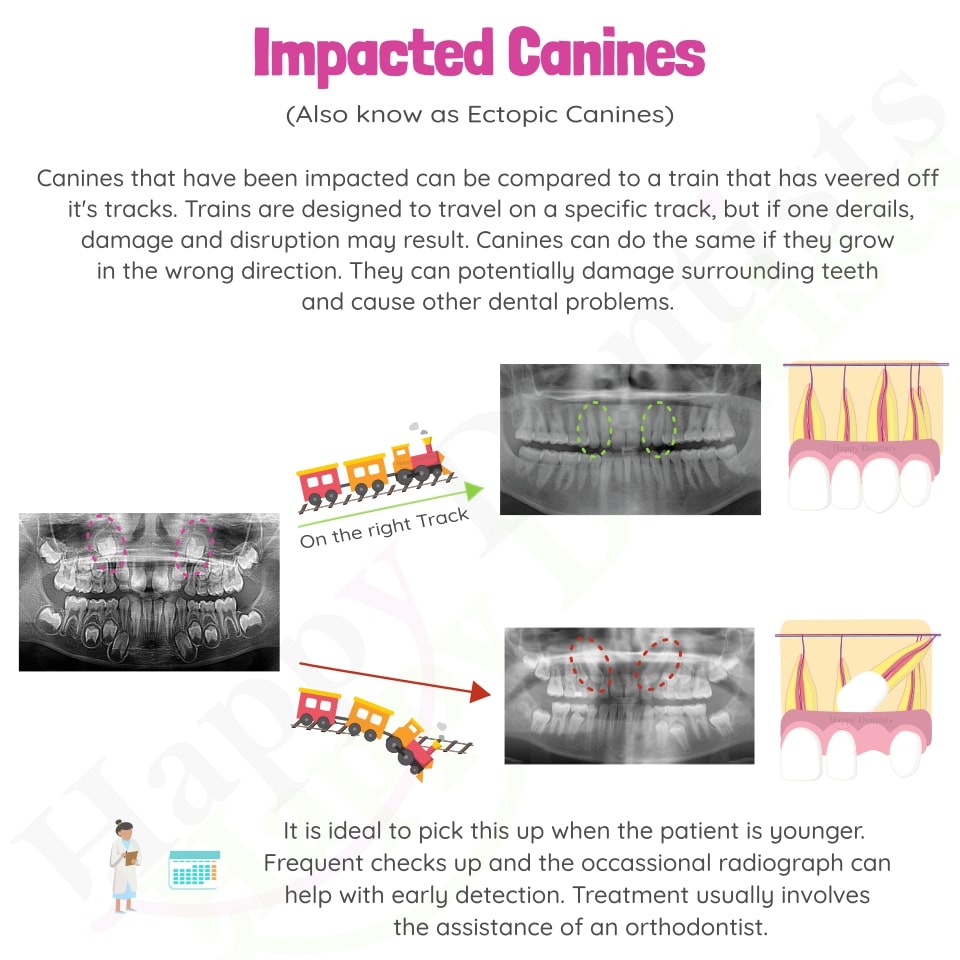
About Impacted Canines
The Maxillary (Upper) Canine is the most commonly impacted
tooth, when the 3rd molars are excluded. Other teeth to
commonly be impacted are second premolars and lateral
incisors.
Classification
The impacted canine can be classified as buccal, palatal or
in the line of the arch. The classification can help with
understanding the possible cause.
Palatal impaction which is the impaction on the roof of the
mouth. This is more common. There are currently two main
theories which explain palatal canine impactions.
1. genetic - because it is often associated with other
dental anomalies (missing premolars, lateral incisors, peg
laterals, enamel hypoplasia), familial aggregation and sex
difference (more common in females)
2. guidance theory - canine erupts along the root of the
lateral incisor, which serves as a guide, and if the root
of the lateral incisor is absent or malformed, the canine
will not erupt.
Labial impaction is more likely related to crowding.
Diagnosis
Early diagnosis and intervention could save time, expense,
and more complex treatment. It is based on both clinical and
radiographic examinations from you local oral health
practitioner.
Before 9-10 years old
Your oral health practitioner will start to palpate for the
canines around 8-9 years old, as well as assessing the
contours of the bone, mobility of the primary teeth; space
available, morphology and position of adjacent teeth. This
is because most maxillary canines erupt labial to the
adjacent teeth at 11−12 years (earlier in females than
males)
After 9-10 years old
Around this age, the oral health practitioner may do a
radiographic exam especially if the canines are not palpable
labially, there is delayed eruption or proclination of an
upper lateral incisors. This is to help localize the canines
relationship with the midline and adjacent teeth, assess any
possible pathology (resorption, cyst). As well as helping to
access for surgical treatment and proper direction for
application of ortho forces. There are a few radiographs
that may be taken depending on the case.
PAs or OPG
Most Commonly used to assess the location of the canine and
possible impaction. This can be done using 2 peri apical
radiographs with a slight shift or an OPG and an occlusal
radiograph.
Frontal and Lateral Cephalograms
Frontal and lateral cephalograms - can sometimes aid in the
determination of the position of the impacted canine
relative to other facial structures (e.g., the maxillary
sinus and the floor of the nose).
Cone Beam Computer Tomography
Complex and severe cases or when surgical exposure is
required - cone beam computed tomography. However, increased
cost, time, radiation exposure, and medicolegal issues
associated with using CBCT limit its routine use.
Management
No treatment if the patient does not desire it.
There is always the option to do nothing. Which depending on
the location, the age of the patient and difficulty to get
to may be a valid option. This will need to be discussed
with your orthodontist and oral health practitioner and
understand that there is the risk of resorption to other
adult teeth and cyst formation. Furthermore in most cases
baby canine root will eventually resorb and it will have to
be extracted, meaning this may affect your smile and may
need to look at replacement options (which is discussed
further below).
Extraction of primary canine if good likelihood of tooth
erupting from age 10-12 years
The likelihood depends on a few factors such as an open
apex, angulation, position (high, mesial, distal). The
prognosis is further improved if the removal of a physical
barrier is required like a supernumerary tooth, odontome
etc. Furthermore if the creation of sufficient space by
maxillary expansion and molar distalization improves the
prognosis of canine impaction If the canine fails to erupt
or improve within 12 months, the orthodontic treatment will
most likely be exposure and alignment (discussed below)
Surgical exposure & ortho tx to bring tooth into line of
occlusion
This method is used when the above technique doesn't work,
cant work or after complete root apex formation.
If the impacted canines need to be surgically exposed, pt is
often referred to specialists such as orthodontists & oral
surgeons. It can be either managed via open exposures or
closed exposures. Labially impacted canines should be
treated by closed exposure to prevent the eruption of tooth
through non keratinised tissue. Where as palatally impacted
canines can be managed by open exposure because the hard
palate is covered by keratinised mucosa.
If there is insufficient space for the exposed canine
to be aligned in the maxillary arch, an appropriate
treatment plan (which addresses all orthodontic problems)
should be followed to achieve acceptable occlusion. Please
beware that their are xommon complications that include the
following: root resorption, bone loss and gingival recession
around the treated teeth
Extraction of impacted canine
This is often not preferred because it may complicated and
can compromise the ability to provide the patient with a
functional occlusion. However, this may be considered if
there are pathologic changes (e.g., cyst formation,
infection, canine/adjacent teeth are undergoing external or
internal root resorption)
Options after extraction
Prosthetic replacement of the canine. (Dental Implant or
Dental Bridge)
Movement of a first premolar in its position.
Posterior segmental osteotomy to move the buccal segment
mesially to close the residual space
{kind=link}
{kind=link}
{kind=link}